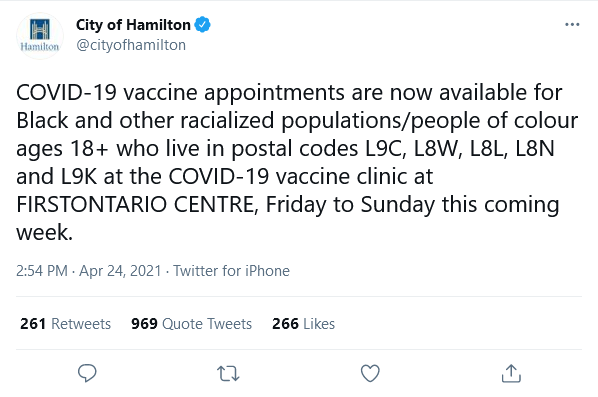
It’s hard to believe that officials in Hamilton, Ontario, one of Canada largest cities, didn’t hear the faint clanging of ethics alarms when they came up with this policy.
The CBC reported that public health officials pressured the agency to “prioritize racialized, disabled and low-income residents.” I think “racialized” is a cool euphemism, don’t you? How does one get “racialized”?
75% of Hamilton’s population is white, but non-white communities have accounted for nearly half of all pandemic cases in the city.
Your Ethics Alarms Ethics Quiz of the Day:
Is Hamilton’s policy ethical?
I’m amazed no city has tried this in the U.S.

Who says they haven’t tried it here? I’ve heard “prioritize populations of color, who are disproportionately impacted.”
I think it would be ethical to vaccinate the most at risk groups first, but I find it dubious that these groups are just non-white people period. I am sure socioeconomic factors, or geographic distributions are more relevant factors. They should have said residents of 01234 area codes with lower incomes, food stamps, etc are eligible, so on and so forth. But just saying “all except whitey” would probably run afoul of anti-discrimination laws, which I would guess are more intense than the US counterpart laws.
In conclusion, this race discriminatory vaccination opening is unethical and reeks of affirmative action style race-based decision making, which is wrong.
Reserving appoints for hard-hit zip codes is unquestionably ethical. Targeting vaccine advertising for hard-hit zip codes is unquestionably ethical. Reaching out community organizations in hard-hit zip codes to encourage their members to get vaccinated is unquestionably ethical.
All of these perfectly ethical strategies dance around the fact that the zip code has a population particularly vulnerable, who in addition to their heightened risk likely also share a minority racial identity.
The campaign targets a vulnerable population, which is ethical. It is also blatantly discriminatory based on race, which is unethical. This campaign is certainly honest though about it intention to target racial minorities hard hit by the virus. That is a utilitarian point in its favor. The same goal could be achieved with cute but meaningless racially-neutral language. Deceit is unethical.
I have no idea how large zip codes in Canada are. Perhaps they are so large as to be meaningless in targeting a specific vulnerable population. Placing a racial requirement to reserve the vaccine for those in a zip code in most need may be the least unethical option to get a limited resource into the arms of who need it the most.
The studies done seems to show that there is no racial component to COVID outcomes. The ‘Minorities are more vulnerable to COVID” narrative is a myth.
https://www.montefiore.org/study-finds-no-racial-disparity-in-covid-19-case-fatality-rates-at-montefiore-when-controlling-for-key-risk-factors
Seattle and Vermont had vaccinations for minorities only. Michigan put black residents before the elderly. The CDC has a tool called the Social Vulnerability Index (SVI) to triage distribution of the vaccine and it puts race before age, economic status, and health risk factors, so it is likely that most states are doing it.
From the article: “The study results suggest that, across racial and ethnic groups, higher mortality rates were primarily driven by older age and the presence of multiple comorbidities, including chronic diseases such as obesity, diabetes and cardiovascular disease that are prevalent in Black and Hispanic communities served by Montefiore | Einstein.”
[Query: When did obesity become a ‘chronic’ disease? Does obesity enter the host via any access point other than the pie hole?]
I suspect there are a fair number of First Nation people (or whatever the current Canadian equivalent of Native American may be) in Hamilton.
Clearly, Covid is and has been from the outset a disease that kills the elderly and the sickly, particularly the sickly elderly. Has anyone done any thinking about the ethics of unprecedentedly suppressing entire populations and economies to extend the already limited, fragile lives of certain elderly and sickly? Pneumonia and seasonal flus kill millions each year. Why haven’t we shut things down in response to these infectious diseases until there is a cure? This has been my concern all along. I remain convinced that when this whole over-reaction to Covid is analyzed coolly and in retrospect, it will go down as the most massive public health and economic policy disaster of all time.
I’m interested to know why black residents in Canada are considered at risk. Isn’t the narrative here in the U.S. that the black population is at risk because of lack of access to medical care (due to racism or something?). Don’t citizens of Canada have taxpayer-funded medical care? Why would black residents there be considered more at risk than white residents if they all have access to so-called free health care?
Am I missing something?
Oh, yes, restricting vaccine access based on race is definitely unethical.
I am on the fence. Perhaps it is an ethical vaccination program that got sideswiped by “inclusion and equity” policies, which landed in unethical results. Though, that does beg the question of whether the result is determinative of the ethics of the program or policy. I am sure it is a rationalization on Jack’s Rationalization List – ends justify the means? Do the means justify the ends? The brain simply boggles.
jvb
Diseases are racist. That is the only conclusion you can make based on the data. Why would a virus preferentially target every racial group in the world except caucasians? OK, it may randomly happen with one, but why does this happen to ALL diseases? They all must be racist. The only other options are that ‘white’ culture is healthier than all other cultures or that our news media reporting and government pronouncements are lies told to fit a narrative. We can be pretty sure the latter is true.
Clearly these bacteria and viruses are systemically racist.
There is all kinds of hand wringing by the leadership (chough cough) in Oregon about the vaccination rates among minorities. They haven’t created any kind of special access like Ontario did. I’m failing to see how there is any racism behind this as until recently the vaccines were distributed by the state. Recently they’ve added private pharmacies, but until then the distribution was managed by the state, regional government for the Portland area, and the counties by the rest of the state. There is zero cost to anyone if they get if from the government clinics, and only a dosing fee from a private pharmacy.
Apparently making people get off their hind ends and motivate themselves to one of the clinics is racist.
The goal, as several commentators have pointed out, is to deliver vaccines to populations most at risk of contracting COVID-19. In Ontario, vaccines are still quite scarce and a third (and most severe) wave has filled many urban ICUs, so prioritising key groups is very much to the public’s benefit.
Generally speaking, in Hamilton and area, minorities disproportionately live in multigenerational households, are low-income essential workers (eg fast food as opposed to healthcare) and/or are of lower socioeconomic class (which associates with fewer sanitation resources, lower health literacy, etc). I can see the benefit of using the criteria of “18+ and racialised” for the sake of simplicity, even if it is racial discrimination. I personally suspect (as Jack and several others do) that discrimination did not bother Hamilton Public Health as much as it should have, but I’m willing to give them the benefit of the doubt.
That said, I’d hate to staff one of these priority clinics. I assume they must operate on the honour system, but I can’t help but imagine staff holding FItzpatrick skin tone scales up to people to determine their eligibility.
Surely Dr. C, all a patient would have to do is “identify” as having been “racialized.”
I fear anything more would be TRUE RACISM.
Crazy idea: How about something other than the color of one’s skin to tie between risks of covid and the vaccine? Many of the characteristics ascribed to racism can better be tied to economic classifications. How about job category, location, etc?
Better than telling the poor white person working shoulder to shoulder in a food processing plant that they don’t deserve the vaccine because they’re white, but those on either side of them do.
That was my point above. There is no link between race and COVID infection or outcomes.
Unrelated point: If the insurance industry finds that a certain population group gets into car accident and is injured more than other groups, do we assume cars, roadways, and traffic laws are biased against them? Do we give them breaks on their auto insurance to even out this discrimination and have government subsidies for them to get safer cars and SUV’s?
It’s far too late in the game for this to make any difference in the outcome, so what we have here is political virtue-signaling. Imagine that.
If there had been a serious attempt to provide vaccinations to the most vulnerable in the general population (excluding medical personnel in ACTUAL CONTACT with Covid patients, not the guy in accounting), the prioritization would have been:
1. The obese. By degree.
2. The old. By age.
3. Household density, including institutional residents.
In Ontario, vaccines had indeed been offered to the elderly first; depending on the area, those 40+ are now eligible for vaccines. This Hamilton program runs parallel to existing age-based vaccination programs.
I would also say it’s never too late (except to close borders)! Decreased community spread is decreased community spread. We can debate how best to do it, but I doubt anyone could reasonably argue against its merits.
The plain meaning of racialized is ‘categorized according to race’, so, everyone’s included, and therefore no problem in targeting postal codes where there is a high preponderance of at-risk people, right?
But, in Canada, racialized generally refers to non-whites, with First Nations peoples sometimes included, sometimes not. So, now, it’s by race and not by risk, and, yes, that is unethical.
By now, the risk factors are well known, and prioritizing by those would be ethical, though problematical. Imagine, “Hop on this scale, sir, and let us see just how grossly obese you are.” Or, “Show me medical evidence that you are diabetic.” Or, “Let’s have a look at your latest pay stub showing you’re a front-line health care worker.”
With no good option in sight, the City chose one they considered less bad, certainly knowing they would be criticized no matter what.
I fail to see the problem with prioritizing by risk factors. If you are at risk because you have a problem, why should you be upset about some temporary worker at a vaccination site knowing about your problem or where you work? I think it’s a heck of an idea. Governments should have been telling at risk people to hide out right from the start, instead of telling everyone to shelter in place.
I don’t disagree, Bill. I was trying to see it from the viewpoint of the woke folks in Hamilton.
But Jeeze, Ed, these wokesters are the same people who insist Covid is worse than the Bubonic plague and Republicans controlling any branch of the government, combined and that it’s all about SCIENCE and people doing what they’re told by their superiors. Sheesh.
Early in the pandemic response, I read my state’s (Tennessee) COVID response plan, including the early drafts of the vaccination plan. Apparently each state had to submit a plan to the US Department of Health and Human Services, and each plan had to address many specific areas. Among these areas was (paraphrased) ‘How do you plan to identify and reach critical populations?” “Critical populations” included many categories of people, mostly the various age groups, vulnerabilities and occupations that we have seen reflected in the different “phases” of vaccine administration, but also included “People from racial and ethnic minority groups.” Our state plan was somewhat vague on the answer to that question but basically proposed identifying and reaching ethnic and racial minority groups using information from the State Office of Vital Records and Statistics, US Census data and the CDC Database. I was curious as to how that might play out in practice, but during the various announcements of vaccine availability/eligibility I never heard a mention of minority groups. Of course, my county is 91% white so maybe no special effort was needed to reach our small number of minority citizens. Each county’s office of the State Dept. of Health was in charge of vaccine distribution for the county, so procedures surely varied somewhat from county to county.